



Theme 3: Measuring the improvements
What does measuring the improvement mean for the Northern Health and Social Care Trust? It is about exploring more reliable and accurate means to measure, value and report on quality improvement and outcomes. During 2023/24, each Trust was required to measure a number of quality improvement indicators, and listed below are some examples of measuring the improvement.
Healthcare Associated Infections (HCAI)
Clostridioides difficile
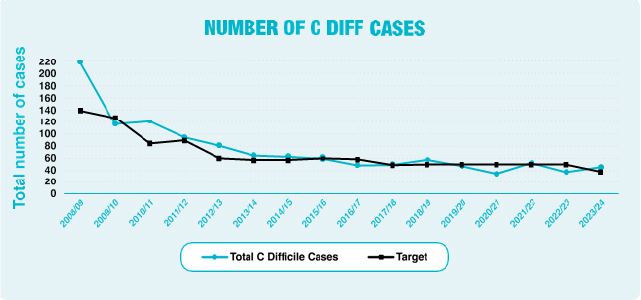
Clostridioides difficile, formerly known as Clostridium difficile (C. difficile), is a bacterium that some people may carry in their bowel and is normally kept under control by good normal gut bacteria. Certain antibiotics can disrupt the natural balance of bacteria in the bowel, enabling C. difficile to multiply and produce toxins that may cause mild to severe illness, including symptoms of diarrhoea. C. difficile bacteria are able to survive on surfaces for long periods and are easily transmitted via contaminated hands, equipment and environmental surfaces.
The Trust performance on C. difficile infections at the end of March 2024 was 45 cases against a target of 37; at year-end this was above the target set by the Public Health Agency (PHA).
MRSA
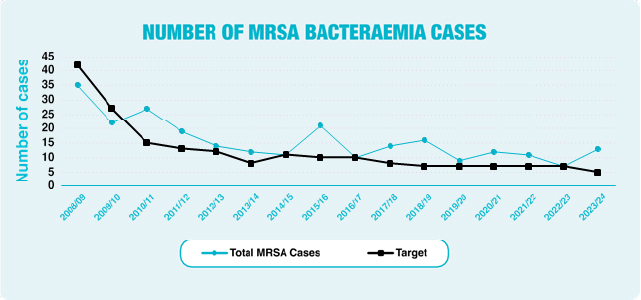
Methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia is a type of bacterial blood stream infection that is resistant to a number of widely used antibiotics. As a result, it can be more difficult to treat than other bacterial infections.
The Trust performance on MRSA bloodstream infections at the end of March 2024 was 13 cases against a target of 5; at year-end this was above the target set by PHA.
Safer Surgery/World Health Organisation (WHO) Checklist
The World Health Organisation (WHO) Surgical Safety Checklist is a tool used by clinical teams to improve the safety of surgery and reduce deaths and complications. The checklist was designed to reduce the number of errors and complications resulting from surgical procedures by improving team communication and checking essential care interventions. During 2023/24 the Trust achieved 92% compliance with the WHO Surgical Checklist.
The Band 6 Clinical Sister in each area completes WHO audits monthly. There are also three-monthly observational audits carried out where the Clinical Sister will observe all practices within the theatre environment. Each department manager also conducts an audit in another theatre department to assess compliance. Compliance with these three-monthly observational audits for 2023/24 was 97%.
Maternity Services
Within the Trust, a new model of care was introduced in July 2023, where all inpatient and birth provision was relocated to the Antrim site. The Trust is committed to enhancing the Causeway Maternity Hub by improving local access to antenatal and postnatal services for women within the Causeway locality. Complex antenatal clinics have been moved to Causeway so as to mitigate the distance women have historically been asked to travel to receive this care.
Perinatal Mental Health/Social complexities
Alongside previous obstetric led antenatal clinics, there is a dedicated perinatal obstetric clinic. Since the reconfiguration of services, the community perinatal mental team commenced two weekly clinics in the hub. This has facilitated an improved pathway and increased co-ordination in care between the multidisciplinary teams.
The Trust has established various complex antenatal care pathways to facilitate increased access to services, these include:
- Third trimester Midwifery Led Scanning
- Weigh to Health Pregnancy for women with an increased BMI in pregnancy
- Social complexity clinic
- Specialist infant feeding clinic
- Maternity Care Clinic
Pathways are currently being developed and will be launched in the coming few months to provide a cohort of risk-assessed women to receive follow up antenatal care who present with gestational diabetes; further increasing perinatal services to the women in the locality of Causeway without the need to travel to the Antrim site.
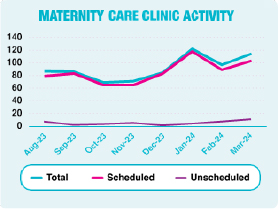
Maternity Care clinic
The Maternity Care clinic is a dedicated provision for scheduled care and a limited number of unscheduled care provision. Since the opening of this unit, 733 women, until end of March, have benefited from the utilisation of this service. The table below highlights the encounter types which have been completed in the woman’s local area without the need to travel to the Antrim hospital site.
Scheduled care includes iron infusions, caesarean section pre-operative care, screening tests, including those for diabetes and fetal and maternity wellbeing checks to name a few. Unscheduled care can include assessments of blood pressure and assessment if spontaneous rupture of membranes may have occurred.
Maternity, Continuity of Midwifery Carer (CoMC)
Continuity of Midwifery Carer (CoMC) is a regional transformation service change aiming to build professional relationships between women and their care providers. Care is provided by a small team of known midwives through the antenatal, intrapartum and the early parenting period. The Lead midwife for continuity of midwifery carer is working in partnership with the regional leads to ensure safe, robust implementation and contingency planning is undertaken within the Trust. A phased accountability approach will be utilised for the transformational service change with the development of small teams eventually leading to CoMC being the ‘default’ model of care. The Trust were the only Trust in the region who had an established CoMC team from 2020, the Lotus Team. The Team has since aligned with the regional model in 2023 and can demonstrate improved clinical outcomes, for example breastfeeding initiation rates are increased from the traditional model of care. The Care Opinion platform is a testament to the positive impact the Lotus Team have had on the experience of maternity care within the Trust. Some excerpts from Care Opinion:
“My anxiety and stress levels were so high until I met with the Lotus Team. They made me feel at ease and were always there at the other end of the phone if I needed extra support”
“….can honestly say if it wasn’t for the help from lotus my pregnancy would have been very different”
“I feel happy to have had such a great team. I would say to anyone expecting a baby please, please consider the Lotus team”
“The Lotus team were beyond amazing during my pregnancy and labour! They had made me feel so comfortable and at ease throughout the whole thing!”
“My lotus midwife was an amazing support all through my pregnancy, labour and after my daughter’s arrival. Longer appointment helped to provide excellent person centred care. She has helped me be more confident and supported me in every single thing”
Succession planning
Succession planning in the field of midwifery is essential to ensure a skilled and capable workforce for the future. There is no recognised model for midwifery succession planning. The Trust implemented the first succession planning programme for midwives in Northern Ireland in 2018. This programme was evaluated positively by attendees with clear outcomes, notably 63% of participants progressing into band 7, 8 or specialist midwifery roles. The clear outcomes provided the impetus to continue with another programme and to expand this initiative to enable all midwives to avail of this opportunity.
In total 22 participants have participated in the programme in 2023 which used a hybrid model, combining face-to-face and virtual sessions over Microsoft Teams in order to overcome any delays or uncertainties relating to COVID-19.
The programme is set to conclude with all participants being offered shadowing opportunities with the Senior Midwifery Team. Following this, key achievements will be evaluated fully, however feedback from participants has been overwhelmingly positive; acknowledging the inspiration and insight gained from guest speakers, and also insight into other roles and an understanding of potential career pathways, previously not considered.
Lessons learned from this programme include recognising the importance of face-to-face sessions amongst participants to create opportunities for further engagement. Plans are in place to review the programme and develop a generic model that can be used in future programmes.
Recommendations include the establishment of a permanent succession planning programme to be included within training and leadership. This model could also be considered within other areas of our service, including gynaecology nurses, to ensure and prioritise a consistent and sustainable approach to succession planning for both nurses and midwives.
Practical obstetric multi-professional training (PROMPT)
The multi-disciplinary PROMPT team have recently expanded their portfolio to include Maternal Critical Care modules and Outside of hospital PROMPT training with Northern Ireland Ambulance Service (NIAS). Both of these new additions focus on the quality and safety of women and families, whilst increasing the confidence of teams to provide enhanced care within the maternity service.
Prevention of falls
‘Slips, Trips & Falls’ remain one of the most common incident types within the Trust during 2023/24.
The National Institute for Clinical Excellence (NICE) Clinical Guideline (CG) 161 states that people aged 65 and older have the highest risk of falling, with 30% of people over 65 and 50% of people older than 80 falling at least once a year.
The number of falls during 2023/24 has reduced to 1,698. The following reasons continue to contribute to these rates:
- Increasing ageing population
- Increasing prevalence of multi-morbidity, polypharmacy and frailty
- Deconditioning of the elderly population as a result of COVID-19 and associated social isolation
The Trust continues to see the importance of falls prevention as a key component to healthy ageing. To facilitate this, the Trust has established a Falls Steering Group focusing on a multi-disciplinary and agency approach to the prevention and management of falls.
Falls Awareness training sessions covering multi-factorial risk factors, continued to be delivered to Trust and Care Home staff by the Falls Prevention team. A number of Regional Falls Awareness e learning modules have also been launched focusing on specific locations for clinical facing staff.
The Regional Falls pathway for care homes has been launched, this includes a guideline for the immediate management of a resident who has fallen. The Trust is continuing to support staff to embed this in practice and continue to offer a falls prevention screening and advisory service to Trust and Care Home staff via the telephone, offering further advice and guidance regarding falls and injury prevention.
The established Falls Screening Service continues to accept referrals via Northern Ireland Ambulance Service (NIAS), the Trust Emergency Departments (ED), Minor Injury Units and Fracture Liaison Service. The service also accepts self-referrals direct from service users. After completion of a multi-factorial falls screening, onward appropriate referrals are made to internal and external services, to help reduce the risk of falls and subsequent injuries.
Within the Trust’s inpatient settings, the FallSafe bundle is embedded into practice, with participating wards completing monthly compliance audits, identifying areas for learning and developing improvement plans.
The Trust also continued to complete post-fall investigations, on all inpatient falls that resulted in a moderate to catastrophic injury. Areas identified for learning and improvement are discussed with ward managers, and shared with Senior Management. Action plans are taken forward within teams to address any gaps in practice.
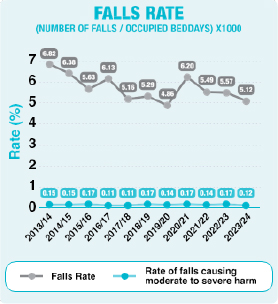
Falls rate per 1000 beddays
The 2023/24 falls rate across all adult inpatient areas was 5.12%, and the rate for moderate to catastrophic harm was 0.12%.
Next steps
- Ongoing Regional Falls collaboration to standardise assessments post-fall within the inpatient setting
- Reduction in inpatient falls will be one of the top 5 key improvement priorities for the Trust in 2024/25
Prevention of pressure ulcers
Pressure ulcers are defined as localised damage to the skin and/or underlying tissue, as a result of sustained pressure or pressure in combination with shear. Pressure ulcers usually occur over a bony prominence, but can be related to a medical device or other object (NPUAP/EPUAP/PPPIA, 2019). Many patients are at risk of pressure ulcers due to multiple co-morbidities and key contributory factors such as, immobility, poor nutrition, weight loss, skin moisture, sensory deficiency, and advancing age.
Pressure ulcers are a major patient safety concern and a quality indicator of care. The Trust therefore, in line with the rest of the region, has a focus on the prevention of pressure ulcers. Preventing pressure ulcers involves firstly, promptly identifying those patients at risk and secondly, reliably implementing prevention strategies for all patents identified as being at risk. In the Trust, this is currently supported by the use of the PURPOSE T risk assessment tool and the inpatient SSKIN bundle:
S – Surface
S – Skin Assessment
K – Keep moving
I – Increased moisture management
N – Nutrition
The Trust have implemented Pressure UlceR Primary or Secondary Evaluation Tool (PURPOSE T) into all adult inpatient and community settings. The Regional Pressure Ulcer Prevention SSKIN Bundles for adult inpatient and community settings were launched alongside PURPOSE T in July 2023. This implementation has resulted in changes to the Nursing Assessment booklet and education tools such as the Pressure Ulcer e-learning programme.
Key facts
During 2023/24, the Trust has built upon the foundations laid in previous years aiming to reduce the number of avoidable pressure ulcers. During 2023/24 the Trust reported 483 hospital acquired pressure ulcers which were graded stage 2 and above. Of these, 152 were stages 3 and 4. Of the total number of Stage 3 and 4 pressure ulcers, 75 were deemed avoidable.
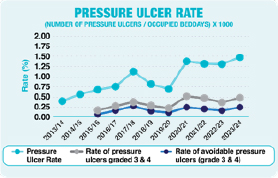
Overall the rate of all hospital acquired grade 3 and above pressure ulcers has increased from 0.35% to 0.46%. The rate of avoidable pressure ulcers has increased from 0.15% to 0.23%. This increase may be reflective of an improved, more robust post-incident review process.
The Wabalogic Medical Photography App has been implemented in hospital settings since April 2023. Staff have embraced the use of medical photography; in Quarter 4, 2023, 71% of hospital Tissue Viability referrals had a supporting Wabalogic image taken at the time of referral. These images support the Tissue Viability Nurse (TVN) to appropriately triage referrals and improve the timeliness of TVN patient advice. In addition to this, the scope of this project now includes the opportunity for staff to capture the condition of patient’s skin throughout their inpatient journey. Over 1000 users have been added to Tissue Viability Active Directory group to date.
Using the Department of Health (DoH) Link Nurse Framework, a total of 70 Tissue Viability Link Nurses have been recruited to support the TVN and the inpatient/outpatient departments in all acute and community hospitals to achieve safe, effective, person-centred wound care. The TVN team hosted a successful link nurse away day in April 2023. A total of 64 Tissue Viability Link Nurses attended on the day from the acute and community hospitals and most of the divisions were represented.
The TVN team have facilitated practical learning sessions in Antrim Area Hospital. Hospital Tissue Viability link nurses and healthcare staff were given the opportunity to practice the fundamental skills of wound care, pressure ulcer prevention and management and subsequently address the key learning themes from pressure ulcer post-incident reviews.
Action the Trust is taking
Quality improvement (QI) initiatives are underway to enhance patient safety in pressure ulcer prevention:
- The contract with Wabalogic is due to end in December 2024. An action plan and a regional consent policy is being discussed at regional illustrative recording meeting in preparation for NIPACs +. The Trust’s TVN lead is working with this group
- All registered nursing staff and non-registered staff working in hospital and community settings should complete the regional e-learning programme for Prevention of Pressure Ulcers in Adults for Registered Practitioners, every 2 years. All non-registered staff including nursing assistants, Health and Social Care (HSC) employed domiciliary care workers and Allied Health Professionals (AHP) support workers can access this HSC e-learning programme
- There are plans to develop a community Tissue Viability Link Nurse group to offer the same opportunity for learning and networking
Action the Region is taking
The Tissue Viability Team actively participates in the Public Health Agency (PHA) Regional Pressure Ulcer Group alongside other Trusts to plan regional strategy, Key Performance Indicator (KPI) monitoring and improvement work in the area of pressure ulcer prevention.
- It is recognised now that healthy women whose labours are prolonged or require caesarean sections are at increased risk of pressure ulcers. Within the Trust, 9 pressure ulcer incidents from July 2020 – December 2022 were recorded. Quality improvement work is ongoing to address this risk. The TVN and maternity department have developed and implemented the Trust Maternity SSKIN bundle including the PURPOSE T risk assessment tool. On worldwide STOP pressure ulcer day 2023, the TVN team and the maternity department celebrated achieving 353 days without a pressure ulcer in the maternity department. Regional collaboration began in 2023 and plans are in place to implement the final version of the Trust Maternity SSKIN bundle regionally, once supporting education has been delivered.
- Safeguarding criteria is being developed regionally to assist staff with decision-making in relation to appropriate referral to the adult protection team following a pressure ulcer incident.
- The TVN team lead collaborated with the regional TVN leads to develop a pressure ulcer definition document. The recommendations in this document are designed to support a more consistent approach to the definition and measurement of pressure ulcers at both local and national levels across all trusts.
Prevention of Venous Thromboembolism
Venous Thromboembolism (VTE) is a condition in which blood clots form (most often) in the deep veins of the legs. This is known as deep vein thrombosis (DVT) and sometimes the clot can travel through the blood circulation and lodge in the lungs causing a pulmonary embolism (PE).
Admission to hospital increases the risk of blood clots (DVT, PE); however, VTE can be preventable. To help prevent VTE in patients admitted to hospitals, a risk assessment is carried out at admission to determine the level of risk of developing VTE, and anti-clotting medicines are prescribed if appropriate.
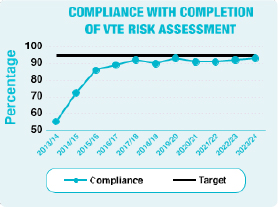
The Trust is committed to achieving 95% compliance with the completion of the VTE risk assessment to ensure patients are provided with the most appropriate and safe care in the prevention of hospital-acquired VTE.
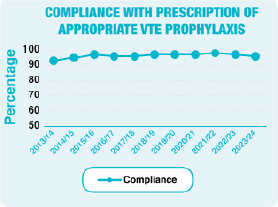
During 2023/24 the Trust achieved:
- 93% compliance with the completion of a VTE risk assessment within 24 hours of admission for patients to acute and community hospitals;
- 96% compliance with prescription of appropriate VTE prophylaxis
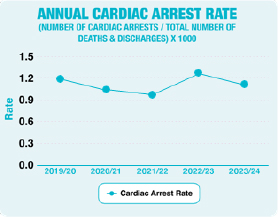
Cardiac Arrest rates
A ‘cardiac arrest’ is where a patient requires chest compressions and/or defibrillation by the hospital resuscitation team. Evidence suggests that the number of hospital cardiac arrests can be reduced through earlier recognition and treatment of patients whose clinical condition is deteriorating. The compassionate care of those patients acknowledged to be nearing the end of their lives may also help to reduce the number of patients treated for cardiac arrests.
The chart below shows the yearly rate of reported cardiac arrests for Antrim and Causeway Hospitals (excluding Emergency Department, Intensive Care Unit, Coronary Care Units and Paediatrics). The Crash Call Rate is calculated as follows:
Number of cardiac arrests, divided by the Number of deaths and discharges, and then multiplied by 1000.
Omitted and delayed medicines
Transforming Medication Safety Strategy Northern Ireland
In September 2020, the DoH launched a five-year plan in response to the World Health Organisation’s Third Global Patient Safety Challenge ‘Medication without Harm’. The strategy involves working collaboratively with healthcare professionals and service users from across Northern Ireland. The strategy sets out four domains, which link to improvement aims and commitments to improve medication safety.
One of the domains relates to HSC staff and is committed to ensuring that staff in our health service have the skills to be medication wise. Omission or delay of medicine doses can lead to harm for patients, particularly when critical medicines are involved such as antimicrobials, drugs for control of Parkinson’s Disease or diabetes.
A monthly KPI, which monitors the number of omitted or delayed medication without a documented reason within inpatient settings, was stood down by the Trust in February 2023. This was following regional guidance from the PHA that it was no longer required. A regional collaboration group was established with nursing and pharmacy to redesign this KPI. Locally, omitted dose medication data was collected weekly for 6 months (January – June 2023) in two acute wards in Antrim Area Hospital. Since then, the omitted medication work has been paused during the regional roll out of the Encompass digital care record. Encompass will change the way that data is gathered and analysed, with significant improvements expected in relation to medication administration. The introduction of the digital Medication Administration Record (MAR) will improve the Trust’s understanding of omitted medication and help to improve care and safety.
Enhanced patient care and observation (EPCO)
For a number of years the Trust has been testing different approaches to improve the care of patients in hospital who experience distress. Within 2023/24, the Trust developed the EPCO model of care. The model ensures that any patient experiencing distress, for any reason, is assessed using a standardised approach, guiding the appropriate level of observation and supporting treatment to alleviate the symptoms of distress (if possible). Part of this model ensures that there is detailed recording of patient behaviour and staff interventions over a 24 hour period, which allows identification of any trends in distressed behaviour, and interventions that help. This is particularity useful when discharge planning as it helps staff to make informed decisions around discharge destinations most appropriate for our patient’s needs.
Insulin
Insulin is one of the top 5 ‘high risk’ medicines used within healthcare which if used incorrectly can lead to serious harm to patients. Around 40% of patients prescribed insulin experience an insulin error during their hospital admission.
The Trust participated in Insulin Safety Week (ISW) which took place in May 2023. ISW is a national campaign to raise awareness of insulin safety, and this year, the Trust Insulin Safety Group emphasised the need for staff to Know, Check, Ask about insulin before prescribing, dispensing or administrating the insulin to a patient.
‘Know, Check, Ask’ is a regional campaign which aims to increase public awareness of the importance of using medication safely, and also to raise awareness among health and social care staff that medication safety is everyone’s responsibility.
Insulin Safety Week
An Insulin Safety Bulletin was developed and issued by the Insulin Safety Group with the aim of raising awareness of insulin-related safer practice. Other resources issued during Insulin Safety Week included a quiz, links to insulin safety educational material, and an insulin safety quiz. The Trust Insulin Safety Card was also distributed to staff during Insulin Safety Week, to provide guidance on dosing schedules for the majority of insulin types available.
Hypo Awareness Week
Hypo Awareness Week (HAW) is a national campaign to raise awareness of hypoglycaemia. According to the 2019 National Diabetes Inpatient Audit, 1 in 4 patients with Type 1 Diabetes admitted to hospital experience an episode of hypoglycaemia during their inpatient stay.
For HAW, the Diabetes Team developed a learning bulletin which was issued to staff across the Trust. Pharmacy staff delivered a training presentation to pharmacists and pharmacy technicians during HAW.
The Trust issued a number of educational resources to staff to mark Hypo-awareness week 2023:
- Hospital Hypos e-learning module (developed by Cambridge Diabetes Education Partnership).
- a hypoglycaemia educational video on preventing hypos in hospital
- updated training/educational materials were uploaded to the Diabetes Section on Staffnet for staff to access readily.
- wards were encouraged to audit the contents of their ‘Hypo box’ to ensure all the necessary treatments are contained within.
Medicines reconciliation
In line with the DoH Medicines Optimisation Quality Framework, ‘Medicines reconciliation, as defined by the Institute for Healthcare Improvement, is the process of identifying an accurate list of a person’s current medicines and comparing them with the current list in use, recognising any discrepancies, and documenting any changes, thereby resulting in a complete list of medicines, accurately communicated. The term ‘medicines’ also includes over the counter or complementary medicines, and any discrepancies should be resolved.’
The Framework also states that ‘patients should have their medicines reconciled by a trained and competent healthcare professional, ideally by a pharmacist’; this should occur within 24 hours of admission. This has been shown to reduce omitted medicines and the patient’s length of hospital stay. During 2023/24, 70% of patients admitted to Antrim and Causeway Hospitals had medicines reconciliation completed on admission.
Regional Pharmaceutical procurement
The Regional Pharmaceutical Procurement Service (RPhPS) assist the Business Services Organisation Procurement and Logistics Service (BSOPaLS) in the tendering of pharmaceutical products for Health and Social Care Northern Ireland, including undertaking contract management activities and the management of shortages. When contracts are tendered, estimated usage data is provided to those bidding for the contract. This data is based on the most recent data at the time of tender advertisement, and is advertised as an estimate that can change. As contracts can remain in place for up to 6 years, the currency of this data is limited, and as suppliers will often plan logistics around the data, it has the potential to lead to short-term shortages.
The RPhPS introduced In-Contract Validation during 2023/24. In-Contract validation was introduced to be an annual process that facilitates a review of usage data for products that have been on contract for at least 2 years and are not going to be reviewed during normal cyclical processes that year, for instance during contract extension or renewal. This process provides data with which we can inform suppliers of significant changes that could impact on the supply chain. Following stakeholder engagement in development of the process, it was agreed that a deviation over 9% could impact the supply chain and therefore should be reported upon. Impacts on the supply chain could result in shortages, which in turn could potentially affect ongoing supply of medicines to patients and introduce new or additional risks, such as administration errors.
In the first annual review (316 product lines from 53 companies), 280 products (88.6%) had usage which deviated from the advertised usage by more than 9%, ranging from -100% to +2660%. All affected suppliers were notified of these changes in annual use, to allow improved planning and supply.
Trust Pharmacy training group
The Pharmacy Education & Training Co-ordination working group was convened to organise monthly training sessions for all pharmacy staff to address gaps in knowledge and learning self-identified by the staff. A survey was shared with all staff and over 50 responses were received. The times suggested by staff and the request for video recordings/training materials to be made available after the sessions to accommodate annual leave and part-time working were incorporated into the programme.
The Pharmacy Education & Training Co-ordination working group has so far provided training sessions on:
- Out Of Hours/Weekend Procurement of Wholesale Items, Cold Chain and Dalriada Urgent Care
- Specialist/Cancer Services Update
- Intravenous Immunoglobulin Update – Prescription, Dispensing and Checking
- Registration of Pharmacy Premises & Role of Responsible Pharmacist
- Supporting De-prescribing In GP Practice
- Opioid Substitution Treatment
- Enoxaparin Video Update
- Registered Pharmacy Premises
- Pharmacogenomics
- Managing Drug Overdose and Illicit Substance
Safer self-administration of medicines
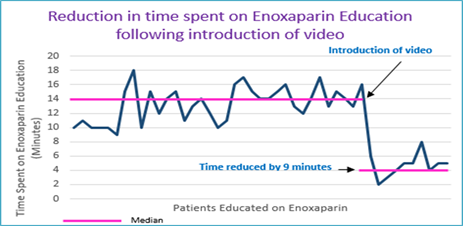
A new education video explaining how to administer an injectable anticoagulant medicine (Enoxaparin) was developed as part of a quality improvement project to help improve patient safety. The aim is to encourage patients to take an active role in managing their medication safely, improve knowledge of their medicines, support healthcare teams in practice and reduce discharge wait times.
The video explains how to self-inject Enoxaparin, why patients are on this medicine and the potential side effects that they may experience. It was initially piloted in the Emergency Department (ED) in Antrim Area Hospital and then rolled out to the Surgery and Maternity units before full roll-out across the Trust.
Results indicate that introduction of the video reduced the time spent by clinical pharmacists by an average of 9 minutes per education session. This time saved has been re-invested into more critical patient-facing clinical activities, including medicines reconciliation on admission, inpatient kardex reviews and participation in ward rounds. A reduction in discharge wait time and re-attendance rate to ED was also observed.
Centralisation of Clozapine service
Pharmacy staff within the Trust Mental Health services worked in partnership with Causeway Pharmacy staff, Mental Health Teams, Transport and the clozapine monitoring company to centralise the dispensing of clozapine across Trust sites to support introduction of Point of Care testing at community clinics using a point of care analyser supplied by the monitoring company. The process also involved transferring prescription information into electronic format to ensure consistency across the Trust and agreement of suitable delivery dates for each patient depending on clinic set up and capacity of the clozapine dispensing service.
At the clozapine clinic, once a satisfactory result is received, the patient is supplied with their clozapine medication before they go home. This is beneficial for both patients and staff as it is a much more efficient way of managing patients requiring intensive blood monitoring for clozapine; testing may be weekly, fortnightly or monthly. Patients now make a single visit to clinic for bloods and receipt of medication instead of two separate clinic appointments. There are currently around 315 patients receiving this service.
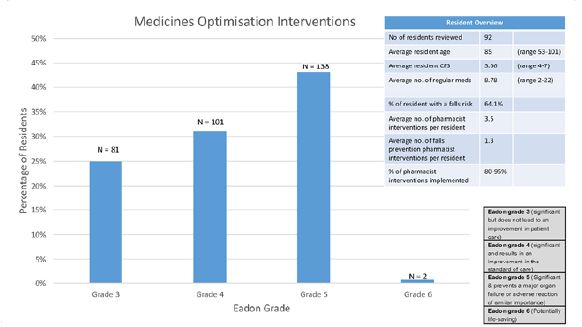
Testing a model of anticipatory care for people living in a residential care home setting, the Pharmacy contribution
In winter 2023/24, the Trust’s REACH (Responsive support, Education and Anticipatory care with Care Homes) team tested an ‘anticipatory care model’ for people living in residential care homes. The model included a medication review and education element, carried out by a Medicines Optimisation in Older People (MOOP) pharmacist.
In total 92 residents had their medications reviewed by the pharmacist. Average clinical frailty scale (CFS) was 5.56, indicating residents were mild to moderately frail. The MOOP pharmacist made a total of 322 medicine optimisation interventions, an average of 3.5 per resident. Of the 322 medicine optimisation interventions, 115 (36%) were in relation to falls prevention, an average of 1.3 per resident. The majority of interventions, 43% were graded significant using Eadon1. The total cost avoidance for the pharmacy element, using the ScHARR model2, equated to an average of £182,000.
The views of capable residents, relevant next of kin and senior care staff involved in medication reviews, were sought via questionnaire; the responses were all positive.
The outcomes of this service evaluation demonstrate the positive impact and value of medicines optimisation for residents with mild to moderate frailty, in a residential care home setting.
- Eadon, H. (1992). Assessing the quality of ward pharmacists’ interventions. International Journal of Pharmacy Practice, 1(3), pp. 145-147. https://doi.org/10.1111/j.2042-7174.1992.tb00556.x.
- Karnon, J., McIntosh, A., Dean, J., Bath, P., Hutchinson, A., Oakley, J., Thomas, N., Pratt, P., Freeman-Parry, L., Karsh, B. T., Gandhi, T., & Tappenden, P. (2008). Modelling the expected net benefits of interventions to reduce the burden of medication errors. Journal of Health Services Research and Policy, 13(2), pp. 85-91. https://doi.org/10.1258/jhsrp.2007.007011.
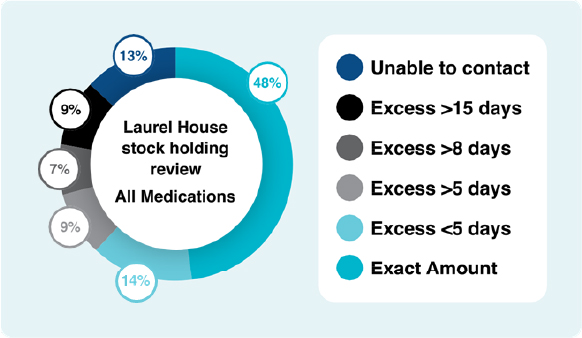
Specialist Services Pharmacy Team – review of patient stocks of oral anti-cancer treatment
Patients who attend Laurel House are provided with supply of oral anti-cancer medications including support medications at prescriber discretion, linked with their next appointment review date. Unfortunately, patients’ appointments and supply can run out of sync. Patients who are admitted to hospital or have treatment doses changed can have insufficient supply to last until their next appointment or conversely have too much medication leading to stock piling or medications waste.
It was decided to review the patients to see the level of stock they had at home, to quantify the level of excess stock holding and ensure the stock holding was in line with the National Patient Safety Agency (NPSA) rapid response document on Oral Chemotherapy (2008) and National Health Service (NHS) standards on prescribing of chemotherapy (2014).
In total, 206 patients had their stock holding reviewed; of these, 48% had the exact amount of stock they required, a further 15% had less than 5 days excess amount. This was usually attributed to the patient preference to have a small excess stock to allow for issues with appointment dates not matching their stock holding, and to manage patient fears of running out of medications.
9% had excess of >5 days’ supply, 7% had an excess of 8 days’ supply and 9% had an excess of 15 days’ supply. Each of these patients were asked to bring their excess stock to their next appointment and their next prescription was adjusted to take account of the excess stock.
The excess stock held by patients and therefore the reduction in the quantity supplied at their next prescription was equivalent to an expected cost saving of £31,619.95. An estimated 25 hours of pharmacist time was dedicated to this project.
Improving the process for ordering of medical gas cylinders
The established process for ordering medical gas cylinders relied on paper records and verbal orders between nursing, portering and pharmacy staff. The process lacked the robust audit trail required for the ordering and supply of a medicine and poor manual record keeping caused significant difficulties for pharmacy to accurately charge gas cylinders to the clinical areas that received them. A change in the legal classification of Nitrous Oxide and Entonox to Schedule 5 Controlled Drug status meant that traceability improvements were required to comply with regulatory and legal obligations.
Corporate nursing, pharmacy, Information Technology and portering staff collaborated to develop an electronic method to order medical gases using the pharmacy stock management system. The order placed on the system by nursing staff in the clinical area prints automatically in the porter’s office, records the details of the requestor, identifies the clinical area and the details of the medical gas cylinder(s) and quantity(s) required. Portering staff deliver the medical gas cylinder to the clinical area and obtain a signature for receipt by an authorised healthcare professional. The orders are sent to pharmacy for charging. This gives traceability through the supply and receipt process. Pharmacy can also see the electronic record of the gas cylinder being requested and can reconcile the paper copies with the orders placed. This ensures the correct clinical area is charged for the medical gas cylinder(s) received and enables timely and accurate charging of cylinders allowing for greater efficiency in stock management of cylinder stocks. The new process has identified the optimum numbers of each type of medical gas cylinders that should be kept on site enabling a cost saving by reducing the number of cylinders ordered by the Trust from the supplier.
Consolidation of stock holding of medical and surgical products
Consolidation of stock of medical and surgical products from each pharmacy department to Tardree House, (Holywell Hospital site) has reduced total stock holding and minimised stock shortages by enabling prompt action in the event of shortages. Phone calls to pharmacy dispensaries and to the procurement department from nursing and ward staff has greatly reduced since the project commenced. Stock suppliers have a single point of contact thereby reducing delivery delays/invoice queries. The project has optimised stock rotation and achieved a reduction in expired stock. Triplication of work (checking/ receipting/invoicing/distributing/purchasing) has reduced across all sites.
Product consolidation has led to the removal of 439 items across the trust (10.1% of the dressings and medical/surgical consumables listed on JAC).
The project achieved an in-year saving of £47,085 (Full Year saving equivalent to £65,757) by consolidation of stock holding and identification of alternative cost effective products.



